Paediatric blast injury studies
Children are seven times more likely to die from blast injuries than adults. But help is at hand.
It's an all too familiar news item: exhausted emergency workers pull a child, alive, from the rubble of a bomb-shattered building. The camera zooms in on the faces of the child’s parents, weeping with joy: in our cosy living rooms, we rejoice with them. But that child’s survival is just the beginning of the story, as those at the Centre for Paediatric Blast Injury Studies know well.
“It’s wonderful when a child is rescued, but if you work in paediatric blast injury, you know there’s a good chance that those child’s legs are going to have to come off,” says Dr Emily Mayhew (MSc History of Science, Medicine & Technology 1999), resident military medical historian at the Department of Bioengineering. “You might see a follow-up story of that child on their prosthetics, dancing and joyful. But you know that in six months’ time, their caregiver may have to make a long, expensive journey to a hospital. Those stumps might have to be re-operated on. Money will have to be found for a new prosthetic, and there will have to be more rehab. The rest of that child’s life will be extraordinarily difficult.”
It is the Centre’s mission to make that child’s life less difficult. Officially opened in March 2023 with funding from Save the Children, it was the logical next step for Imperial’s Centre for Blast Injury Studies, founded in 2011, which addresses the disabling injuries of conflict in adults. “We had to ask: ‘What about children?’” says Mayhew.
It’s a pertinent question, because child victims of 21st century wars are far more likely to suffer blast injuries than those of the 19th and 20th centuries, who were mostly affected by starvation. Wars are now mostly fought in cities – where children live. Their homes are in buildings that are bombed or hit with rocket-propelled grenades. And they also come across explosive weapons such as landmines in the ground, either deliberately left there or left over from previous engagements.
Indeed, the focus on children is vital, says Professor Anthony Bull (Mechanical Engineering 1992; PhD 1995), director of the Centre, for one very simple reason. Children are different from adults, chiefly because they grow. Yet research into child-specific blast injuries thus far has been limited, or non-existent. Bull recalls his experience chairing the expert panel for blast injuries for the Manchester Arena bombing inquiry in 2021 – a terrorist attack in which 22 men, women and children died. “Questions arose that we couldn’t answer because the research wasn’t there,” he says.
Military medical experts in the field can have considerable expertise in treating children, he points out, but they are not set up for it, and their expertise is rarely codified in a way that others can learn from. Examining how blast injury affects growth, for example, requires long-term research: impossible to carry out when trying to cope with the immediate impact of conflict. This led to the publication, in 2019, of the Paediatric Blast Injury Field Manual, by a coalition supported by Imperial and Save the Children – the first comprehensive guide to treating those injuries. “And we published a systematic review, which showed what we knew about children with blast injury, and what we didn’t know,” says Bull. “This led us to the Centre’s research agenda.”
A key part of that agenda is finding new and better prosthetics for that child in the rubble, as well as victims of blast injury, as both will frequently require amputations. It’s a huge challenge that PhD students Caitlin Edgar (MEng Bioengineering 2021) and Claudia Ghidini (MSc Bioengineering 2021) are determined to overcome. Edgar is designing an entirely new, adjustable and affordable prosthetic knee joint for children in low-resource environments. And Ghidini is designing a new socket – the interface between the residual limb and the rest of the prosthetic leg.
“A prosthetic is a life-saving device,” says Edgar. “If you are in a conflict zone, you need your mobility back to flee conflict, to ensure your continued health and wellbeing, and, specifically for children, to get back into education and continue to develop into adulthood. Without appropriate prosthetic care, children will not reach their full potential.”
The two had little child-specific research to call upon. So before they started the design process, they took a step back and created their own body of literature, using case files from Cambodia and questionnaire-based study of children with limb loss in Cambodia and the UK. It gave them crucial insight into the challenges these children face, the impact of the injury, the problems with the prosthesis, and their wishes for the future.
Partnerships are vital: they include work with the Department of Prosthetics and Orthotics in Cambodia, the social enterprise Exceed Worldwide, and the Royal National Orthopaedic Hospital in the UK. There is also emphasis on the extensive expertise of Professor Bull’s group, and Imperial prosthetics spinout GO Assistive Technology.
The pair’s research revealed a multitude of issues. Children with an unsuitable prosthetic can struggle to walk on uneven ground, which is common in conflict zones or rural areas. This can make the leg lock straight, impacting the rest of the body. There is no knee joint small enough to fit very young children. As they grow, the prosthetic frequently needs to be replaced. An ill-fitting prosthetic can cause numerous lifelong problems such as scoliosis and osteoarthritis, as other limbs and joints attempt to compensate.
Similar problems arise with the socket, the interface between the residual limb and the prosthetic leg. “Children told us that they have a lot of issues with pain, as they keep growing and the socket gets tight,” says Ghidini. “This causes problems with the residual limb such as blisters or small wounds, which means they can’t wear the socket. They would like to be able to adjust the leg themselves, so they don’t have an expensive journey to the clinic and miss school – and they would like it to look more like a ‘normal’ leg.”
Ghidini is just about to start her design process, while Edgar’s new knee design will soon enter its first trial. Her improved knee is suitable for children throughout their growth, with an increased range of motion that allows for kneeling. “The leg length can be increased by two centimetres, which might not seem like a lot, but is two to three years’ growth for a child,” she explains. “It doesn’t need cutting or taking apart: it just slides out and can be done immediately and is easily repaired using parts from bicycles.”
Images on right – Sanaa, Yemen, October 2018: Yemeni girls Hala Majed Oqbah (in blue dress) and Aradah Mohammed Oqbah, who both lost one leg in an airstrike while they were playing outside their house in Ibb province, try out prosthetic limbs provided by UNICEF at a rehabilitation centre in Sanaa. Aerial attacks and street fighting took hold of most of Yemen in 2015 and put millions of civilians, especially children, in danger. Credit: Xinhua/Alamy.







New strategies
But developing new prosthetics that work for children also demands fundamental knowledge about exactly what blast injuries do to a child’s body, and how that differs from the same injury for an adult. “First is the injury you can see: the fragments, the bits of rubble that smash into the human being and blow holes in them,” says Mayhew. “But there is also an invisible blast wave which passes through their body and disorders systems at the genetic level. We know from adult studies that this primarily disorders healing: soft and hard tissue, bones and skin. It doesn’t heal. It doesn’t scar. It doesn’t re-form, and it affects people for the rest of their lives.”
PhD student Sumudith Jayasuriya is seeking to fill this key knowledge gap. His work focuses on two different bone growth abnormalities that can follow traumatic injuries. Because child amputees have immature skeletons, bone can grow from their amputated limbs. It’s not just painful and irritating, but also makes putting on and wearing prosthetics much more difficult, which impacts their ability to take part in daily life.
And growth plate disruption, caused by the blast wave, can lead to growth problems. These cartilaginous regions sit towards the ends of long bones in children – when they are damaged, they affect bone growth. “For example, an injury towards the centre of the growth plate can lead to relative shortening of that limb compared to an unaffected limb,” explains Jayasuriya. “An injury to the lateral side of the growth plate can lead to uneven growth, where one side grows longer than the other.” This could lead to the children developing problems such as osteoarthritis or scoliosis or having difficulties performing basic activities.
“We want to use our model to demonstrate that existing prophylaxis are not ideal,” says Jayasuriya. “We also want to explore the effects of different mechanical loading environments, to see if this can reduce bone overgrowth, which could provide a contemporary new therapeutic strategy for dealing with this condition.”
The challenges this team faces are vast – but the potential impact on children’s lives is even more so. “At the Centre, we like to say children are little human beings, not little adults,” says Ghidini. “Everything they need and the problems they face are so different – and so often, they are just forgotten. I hope that we can pave the way for new engineering solutions and rehabilitation methods, reduce pain and give them a better life. I hope we can allow them to just be children.”
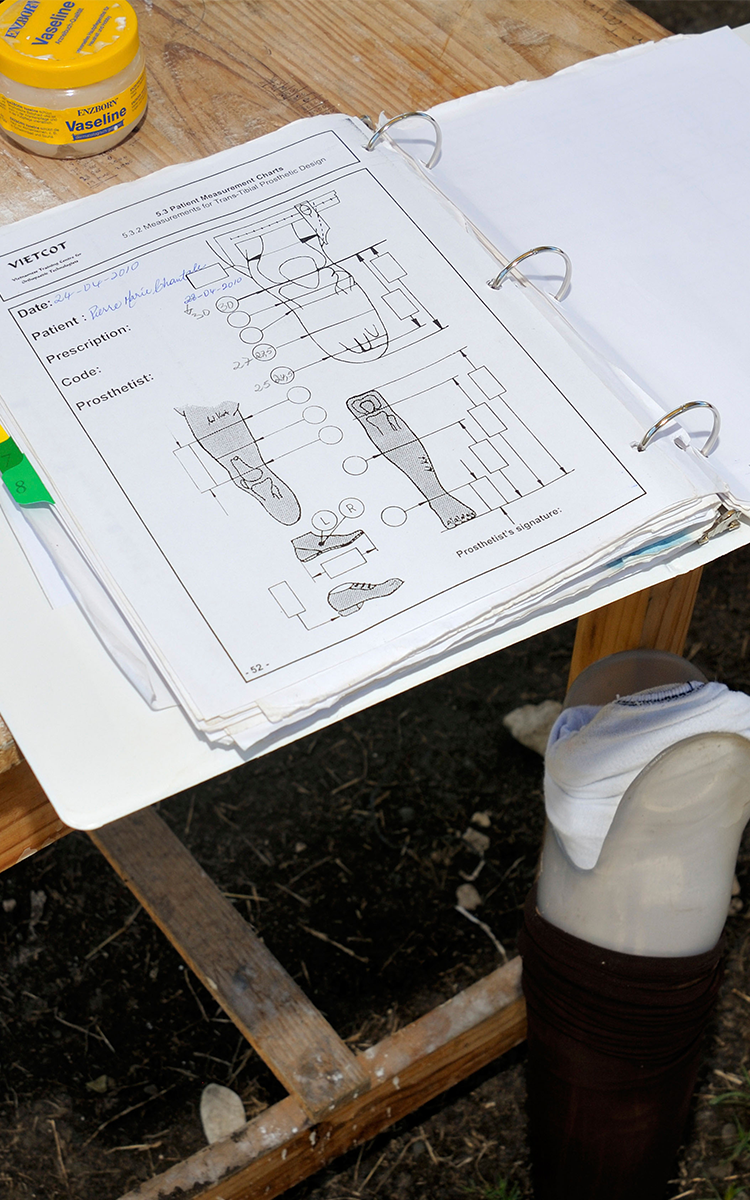
Images on left – Leogane, Haiti, January 2010: Measurements are taken of the stump of a young woman who lost her leg in the January 2010 earthquake, to fit a new artificial limb. Credit: Florain Knopp/Alamy.