Learning from the pandemic in real-time
5 things Imperial's REACT study has taught us


Three million, four hundred and eighteen thousand, seven hundred and eighty-eight.
Since Imperial’s REACT study began little over two years ago, that’s the number of people up and down the country who’ve taken part in the programme, swabbing their noses for the virus or pricking their fingers to see if they’d likely had it before.
That makes it one of the world’s largest coronavirus surveillance studies, and the biggest unique study participant group in existence in the country.
“We really like data,” says REACT director Professor Paul Elliott, from the School of Public Health. “The more data you have, the better you’re able to understand what’s happening, where and to whom.
"And what we gathered is a really precious resource. It’s helped the country become the COVID-19 surveillance envy of the world.”
Getting a study of this size and scope off the ground was a formidable task, especially for a small group that formed virtually overnight as infections with a barely known virus were gripping the country back in April 2020.
“The first thing we did was bring together a fantastic team at Imperial which crossed disciplinary boundaries – epidemiology, statistics, clinical infectious disease, virology, public health policy,” he adds.
“It was the strength and depth of the team's experience that allowed us to mobilise this study so quickly.
“From a standing start, we were up and running within two weeks of our first kick-off conversations.
“It’s remarkable that we were already obtaining swabs on the 1st of May and managed to sample 120,000 people in our first study round.”



They had a helping hand. Ipsos, a global leader in market research, were the study’s logistical partners, dealing with everything from sending out over 17 million invite letters, to organising the refrigeration system to keep the samples cold in transit.
“It’s been the most incredible journey,” says Gary Welch, Research Director at Ipsos. “At the start it was 24/7, we were working around the clock developing and testing study materials to send out to participants, setting up the kit logistics and having Saturday afternoon Zoom calls with the Minister.
“It’s like nothing else I’ve ever worked on and hands down the most rewarding, challenging study I’ve ever contributed to.”
Following the study’s first announcement of its findings in July 2020, it quickly became an eagerly-anticipated source of up-to-date information on the state of England’s epidemic.
“We had three ‘constituencies’ – the Government to inform their policies, the public via the media, and the scientific community, all of whom we were informing in real-time, rapidly, what was going on at that moment in time,” says Prof Elliott.
“We were keen to get our findings out immediately, within a few days of receiving the data from our partner labs. Now our surveillance has ended, we’ll have to go back to the old school way of doing things!”
After two years of data collection, REACT is no longer in the field, but the lights aren’t off for the study.
“With a cohort of over three million people, a key question for us now is which areas of health can also benefit from this work?” ponders Professor Graham Cooke, one of the study’s lead investigators from the Department of Infectious Disease.
“We want to secure a future and legacy of the fantastic contribution that people made to this study,” adds Prof Elliott. “Carrying out further research with this huge group will be enormously helpful to understand the long-term impacts of COVID-19, which is a brand-new disease. Now that we have this resource, we want to make the best use of it for public good.”
While the future of REACT is yet to be written, its legacy is already carved out from the impact it has made on science and understanding of the virus and its consequences. We look back at some of these major contributions, and unravel five of the most important things we’ve learned from the study.






1
DIY: Random self-testing is a valuable tool for population surveillance
Early in the pandemic, testing capacity and availability was extremely limited, reserved for key workers in health and care or people with a narrow set of symptoms that were linked to the infection (fever, new persistent cough, and loss or change of sense of taste or smell). That meant critical uncertainty over the number of people who had the virus but didn’t qualify or put themselves forward for testing, including those who didn’t have any symptoms but were still carrying the virus.
This meant that those being tested gave a skewed and unrepresentative view of the people and numbers infected with the virus. To circumvent this bias, REACT selected people in England randomly to take part, lifting the veil on where the virus was spreading in people who were missed by routine testing.
This was a similar strategy to England’s other major COVID-19 surveillance study, the ONS COVID-19 Infection Survey, but there are key differences. While ONS visited the same people, repeatedly testing households over time, REACT sampled different people in each round of testing. Another key difference was that participants of REACT tested themselves at home, whereas ONS used trained staff to visit people’s homes.
“This has helped shift the thinking to studies and care where self-testing can be considered business as usual for both studies and routine care,” says Prof Cooke.
“Self-testing allows us to do larger, faster, more cost-effective studies, and gives greater control to the people who are engaged in the study.”
Self-testing at home also kept people away from testing facilities and key workers, thus reducing further spread of the virus. REACT used this method to not only detect where the virus was, but also where it had been. These are the two main arms of REACT.
REACT-1 looked at the number of people with the virus, their demographics and where they lived, by swabbing their noses and throats and looking for current infection via PCR testing. REACT-2 used self-administered antibody testing to look for markers of past infection via lateral flow kits.


While lateral flow antigen tests later became a staple in most households, after they were made freely available by the Government for people to check if they were likely infectious, mass antibody testing at the scale REACT achieved had never been attempted before. Soon after REACT-2 was launched, it began testing around 150,000 people every six weeks for coronavirus antibodies. Preceding this was a major public involvement effort to design the information and materials that came with the testing kits, to ensure that people could understand them and carry out the tests correctly. This was run in parallel to a rigorous scientific evaluation of different available testing kits to find out which ones were the most accurate, usable, and available at scale, working with NHS partners.


“This was a magnificent effort, because we were using technology that hadn’t been tested for this purpose before,” Prof Elliott says. “We were able to get information on population antibody levels on hundreds of thousands of people within just a few days; there was no waiting around for test results. This has been a hugely underestimated approach, but we showed its potential as a valuable population surveillance tool.”
REACT-2 yielded insights far beyond tracing the virus’ footsteps in the population, as we will see later.


2
Surveillance acts as an effective early warning system
REACT-1 collected data over a roughly two-week period each month (called a round, of which there were 19 in total). Each of these rounds offered a near real-time snapshot of where the virus was in the population at that time. This provided a vital early warning system, detecting the earliest signals of proceeding surges driven by new variants.
“When things changed very quickly, we picked it up,” Prof Elliott says. “We detected early each successive variant-driven wave, firstly when the Alpha variant began to take over the original strain of the virus. We could see a rise in infections in Essex, Kent and South London as a ‘canary in the coal mine’ marker of what was happening.
“And then when we detected just two cases of the Delta variant, that was one of the first signals that a new wave was coming. Next it was Omicron rapidly taking over from Delta last December, and then most recently the rise of the BA.2 Omicron offshoot in March."
Watch these rises in prevalence from December 2021 to March 2022 in the heat maps below.

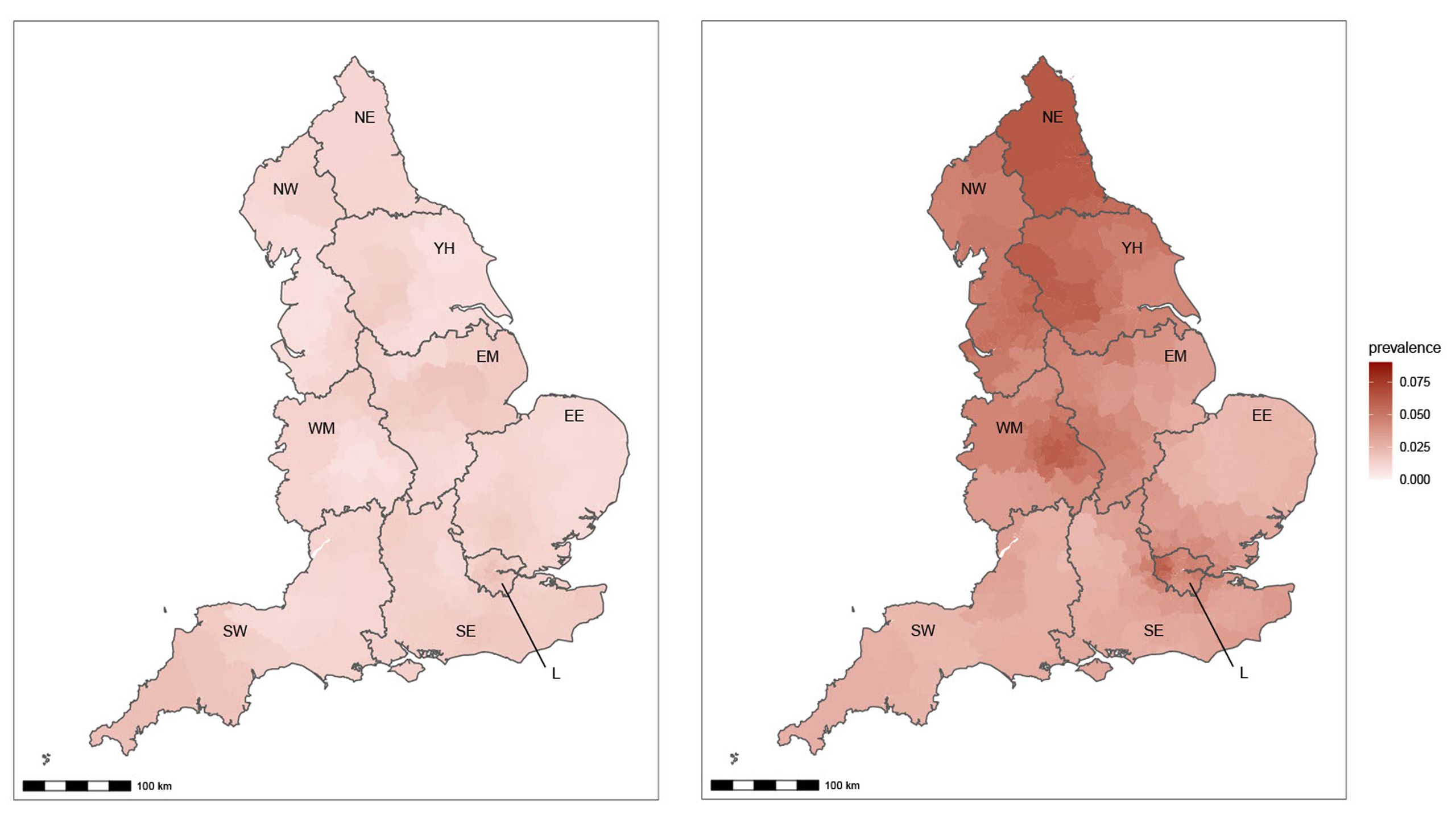

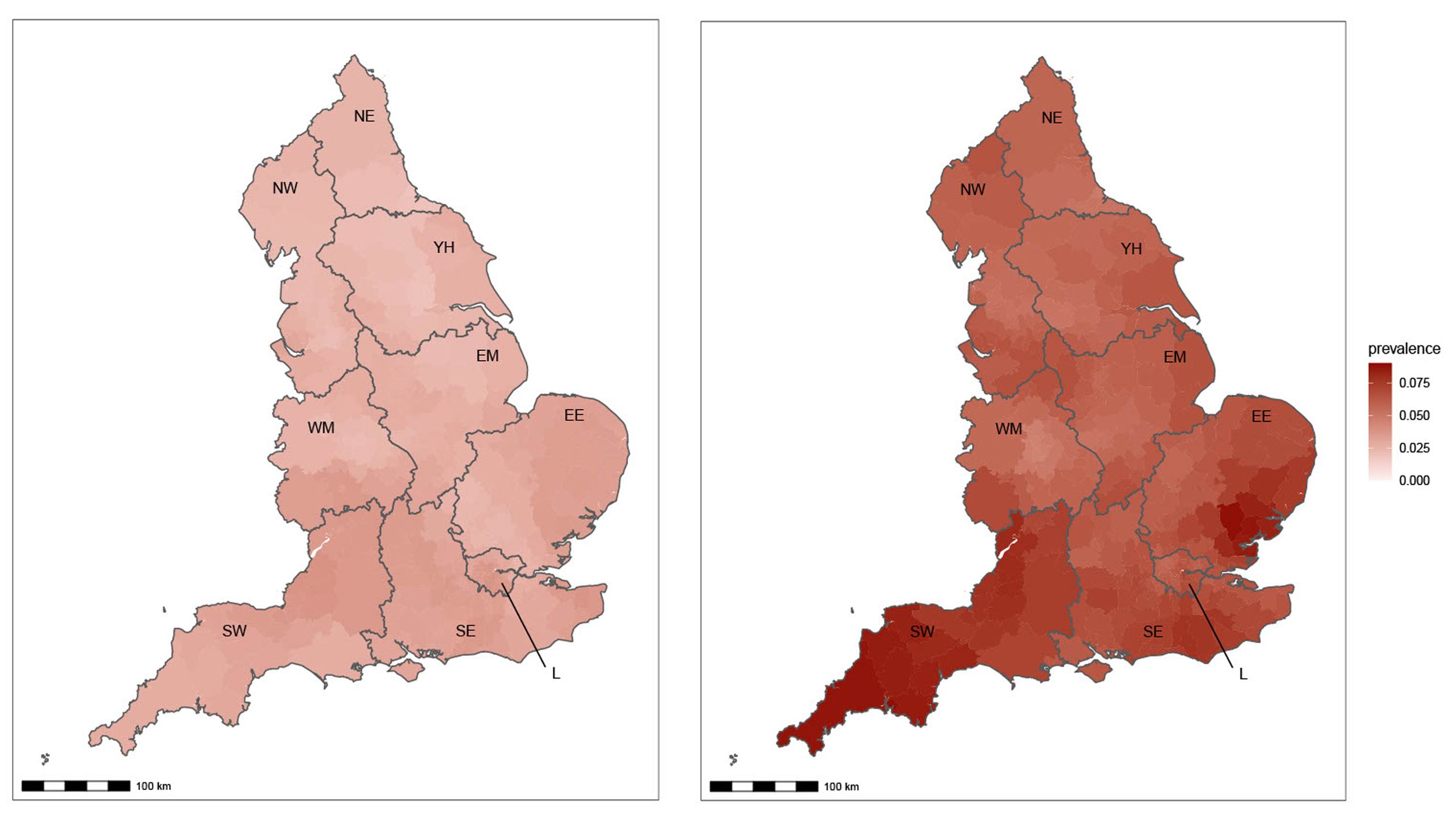
“Each time, we could see these trends happening in our data in real-time," he adds. "And if there’s one thing we’ve learnt from this, it’s that the virus is really unpredictable. Continued surveillance is vital to stay on top of the numbers and spot the next variant if and when it comes along.”
Watch Omicron taking over from Delta below.

By rapidly feeding this information to Government, REACT helped enable policymakers to make evidence-based public health decisions in a timely way. Similarly, by quickly getting findings out to the public, REACT helped people make informed decisions about their behaviours and weigh up the risks of their actions.
3
The impact of the virus has been uneven
Early in the pandemic, it soon became clear that the burden of the virus was not falling on everyone equally. Not just in the UK but in other countries too. People from minority ethnic communities were disproportionately impacted by COVID-19, with hospitalisation and death rates higher in Black and Asian people compared with White people in the UK. This led to speculation about the underlying reasons. Was this because White people had better access to care, or perhaps some biological differences that meant people from ethnic minority backgrounds experienced the disease differently? Both of these ideas were touted, but REACT helped to show that neither were likely explanations.

Antibodies offer a long-lasting record of past exposure to the virus, enabling analyses of the timing and extent of the epidemic. As vaccines weren’t available at this stage of the pandemic, the presence of antibodies indicated past infection and not immunisation. So the team could use data from their REACT-2 antibody survey to look at the burden of infection, and link this to both their questionnaire data covering important demographic information like occupation and household size, and also to hospitalisation and death rates.
Using data until mid-July 2020, the team discovered that the rate of infected people dying – infection fatality ratio – was similar across ethnicities, yet people of Black or Asian ethnicity had two-three-times higher infection rates compared to White people. This was a hugely important finding, suggesting that rather than down to different experiences of the disease or care, the higher burden in minority ethnic communities was likely due to higher exposure to the virus. These trends could be linked to other factors such as people from minority ethnic communities being more likely to live in larger households, or be employed as key workers.
These findings were significant, not only because they challenged the idea of some underlying biological differences, but also because they highlighted the need to work with at risk groups to identify appropriate and effective strategies to reduce these inequalities.

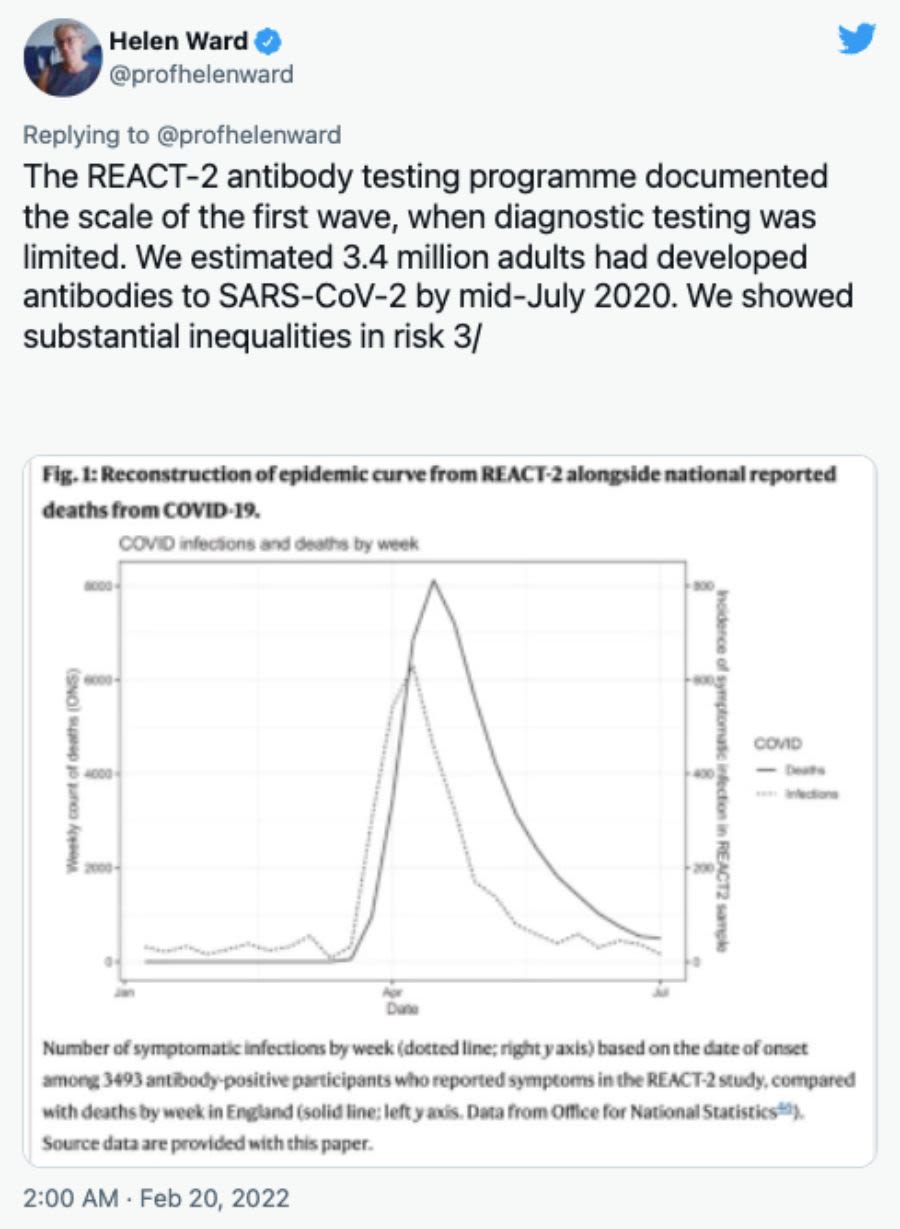
Tweet from Professor Helen Ward referencing this research article published on nature.com
Tweet from Professor Helen Ward referencing this research article published on nature.com
“We’ve been able to identify people at risk and empower people to make decisions on their own behaviours, including whether or not they choose to get vaccinated,” says REACT scientist Professor Christl Donnelly from the School of Public Health.

Prof Donnelly
Prof Donnelly
4
Symptoms are complex, and long-lasting
Until April of this year, the official definition of coronavirus-related symptoms in England included only four symptoms (fever, new persistent cough, and loss or change of sense or taste or smell). If you had any of these ‘classic four’ symptoms, you were eligible for a free PCR test.
“We picked up that this wasn’t telling the full story,” Prof Elliott says.
By looking at REACT testing and questionnaire data between June 2020 and January 2021, the researchers discovered that infection was linked to a much wider range of symptoms than previously thought. In addition to the classic four, chills, loss of appetite, headache and muscle aches were together most strongly linked with being infected. Having any of these, either alone or in combination, was associated with higher risk of infection with coronavirus and the more symptoms people had, the more likely they were to test positive. They also found that the patterns of symptoms differed between the Alpha variant and those of the original strain.
“We’ve been documenting the evolving patterns of symptoms over time and with successive variants and informing policy on how best to define cases,” adds Prof Cooke.
In April 2022, shortly after free testing ended, the official list of symptoms was updated, adding in a further nine that better reflected what the REACT study had been recording.
But it’s not only the breadth of symptoms that REACT has given a better understanding of, but also how long they can last. While some infected people experience no symptoms or mild ones lasting days, others can have debilitating symptoms persisting for many weeks or months, referred to as Long COVID. Some people’s symptoms, like fatigue and breathlessness, are so severe that they can’t work or do many daily activities.
After analysing data on over half a million people between September 2020 and February 2021, REACT showed that over a third had persistent symptoms lasting 12 weeks or more, meaning that over two million people in England may have been affected by Long COVID at the time. When the team carried out further analyses on data from May 2021, the figure dropped to one-fifth of England’s population.
“This represents a significant public health issue that needs to be urgently addressed through appropriate support and treatment,” REACT scientist Professor Helen Ward, from the School of Public Health, said.
A separate arm of the study spun out from REACT to take a deeper dive into Long COVID and still continues. Through detailed profiling of thousands of people’s biological and chemical make-up, the study is answering questions such as who is more likely to be affected, how, and why. “We hope that research moves from describing the problem to developing interventions and treatments soon,” Prof Cooke says.


Prof Elliott
Prof Elliott

Prof Cooke
Prof Cooke

Prof Ward
Prof Ward


5
The impact of vaccination
On 3 December 2020, just nine months after the pandemic was officially declared by the World Health Organization, the UK became the first country in the world to approve a COVID-19 vaccine. Not long after the Pfizer shot was rolled out, Oxford/AstraZeneca’s jab was also given the green light, followed by Moderna. After so many months of loss, fear, upheaval, uncertainty, and change, for many people, this offered light at the end of a seemingly never-ending tunnel of darkness.
Since the rollout of the UK’s vaccination programme, REACT has been on the case, building further evidence on how well it’s working. Although not a randomised clinical trial – the gold standard way of looking at how well a medical intervention works – the REACT study offered important insights.
By comparing infection rates across different groups – such as unvaccinated and vaccinated people, people who had received different numbers of doses, and different age groups who received their doses at different time points – the researchers could estimate how well the vaccines were protecting people against infection.
A second dose cut the risk of infection by two-thirds compared to a single dose, while boosters offered the same reduction in risk compared to two, the scientists found. The protection offered to school-aged children was also stark, supporting the rollout of vaccination to this group.
The researchers also unravelled further clues by looking at antibodies in the blood and linking this to infection rates, and when people received their vaccines. Although the presence of antibodies alone doesn’t necessarily prevent infection, their presence could give an indication as to how protected people are from future illness.
“We were able to show early on the population-level trends in antibody responses to the different vaccines people were receiving, and how these wane over time, possibly indicating declining immunity and the need for booster doses,” says Prof Cooke.
“We were also able to identify groups of people who produced a weaker antibody response, including older people, people with certain pre-existing illnesses, and people with obesity. This highlighted groups who might need earlier boosting, and we fed all of this data into the Joint Committee on Vaccination and Immunisation to help shape the ongoing programme.”


The REACT legacy
“REACT became one of the world’s biggest studies of COVID-19 in the community, successfully tracking the progress of the epidemic in the UK and providing unrivalled insight for policymakers,” says REACT sponsor Professor Ara Darzi, co-director of the Institute of Global Health Innovation.
“It was originally planned to run for one year and the fact that it ran for two, with more findings to come, is testament to its impact.
“REACT gave us regular snapshots of the epidemic at a speed we never thought possible, which is why it became an unrivalled source of information for the Government, the public and scientists, helping us all to make better decisions.
“I’d like to take this opportunity to thank everyone who made its achievements possible – every single participant who volunteered their time to take part, the inspirational research team, our expert partners, and our Department of Health and Social Care/UK Health Security Agency funders.
“REACT’s legacy is thanks to you.”

