The MSk Lab has been involved for some years in researching and building software for joint analysis and surgical planning. We are looking at the basic science of bone and implant shapes and applying it to planning surgery for individual patients.
To do our analysis and planning, we often use 3D models of a patient's anatomy. These often come from CT data, which is excellent for identifying bony structures, or MRI if we want to look at cartilage and ligaments in more detail.
What shape is the hip?
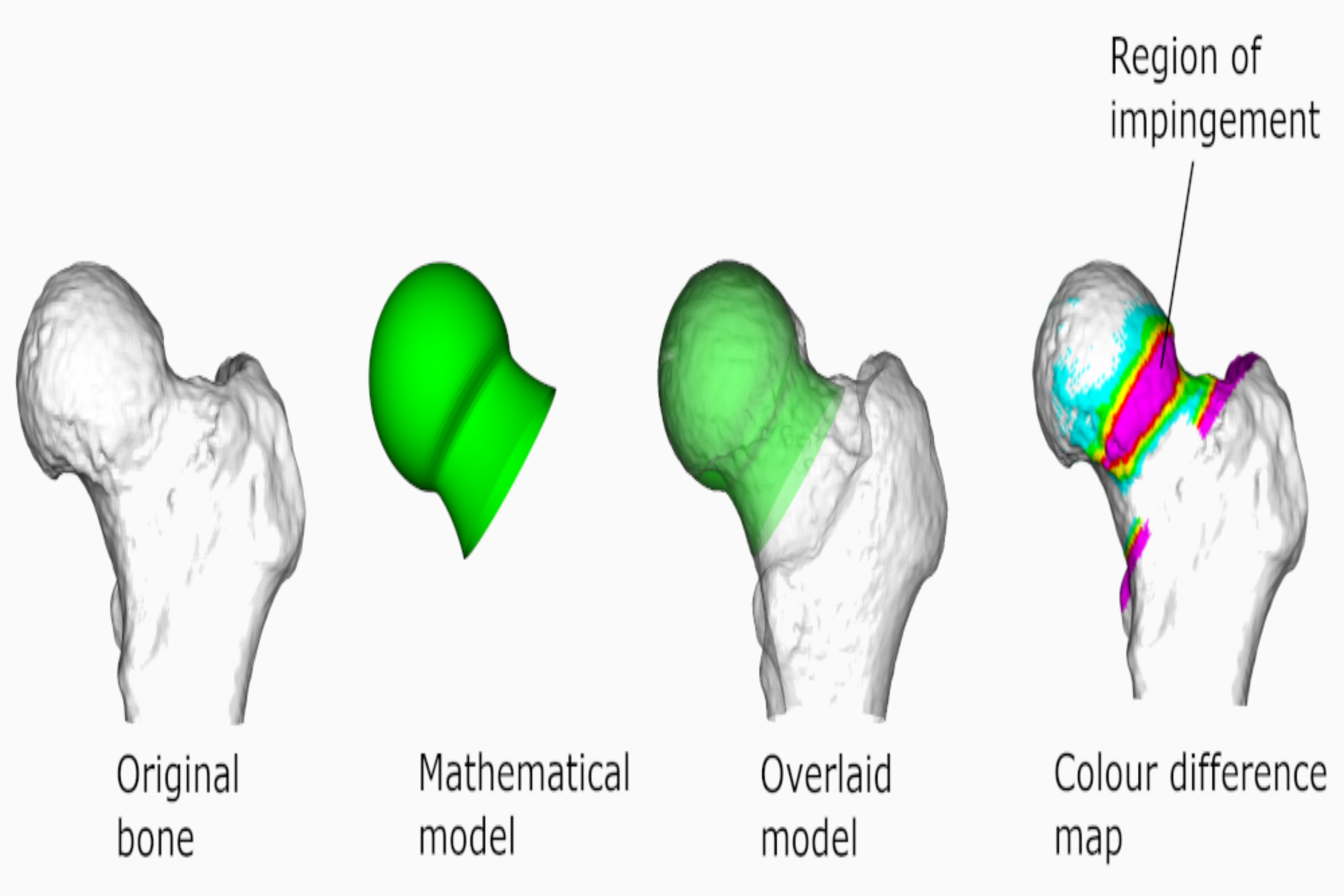
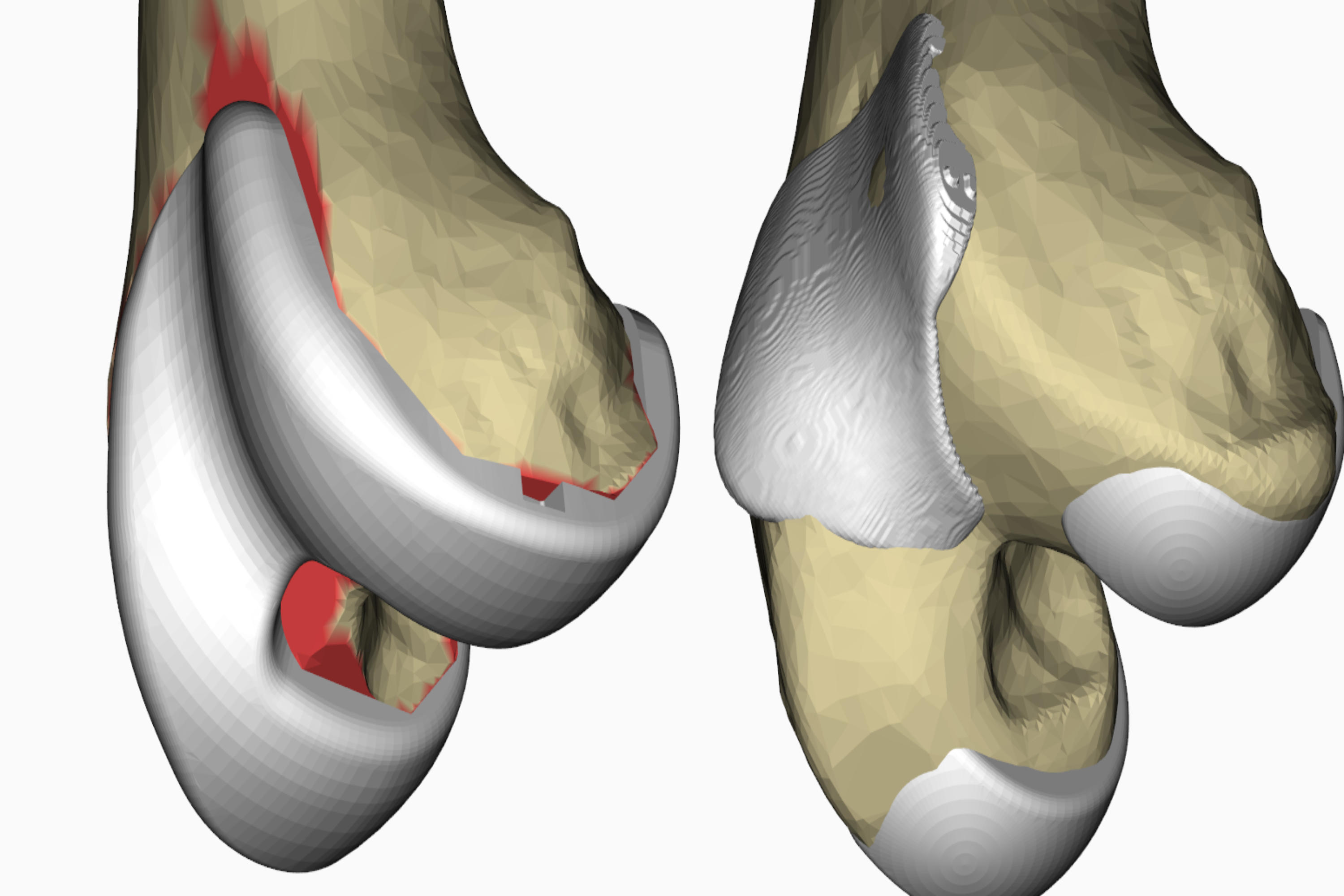
The shape of the femoral head and its relationship to the neck can influence the kinds of problems likely to occur. One problem that we have investigated is that of femoral acetabular impingement, where the front part of the femoral neck prematurely hits the rim of the acetabular cup.
This causes pain, reduces the range of motion of the hip, and the damage caused to the acetabular rim can lead to osteoarthritis. This impingement can be caused by the femoral head sitting too far backwards on the neck or by a bump on the neck itself.
The problem can be reduced surgically by shaving away parts of the neck to reshape it to a more normal geometry.
We developed software to take a 3D model of the patient's femoral head and approximate it to a mathematically ideal shape. We can then determine the difference between the ideal shape and the actual shape to give the surgeon a plan to show which areas of the neck should be reshaped.
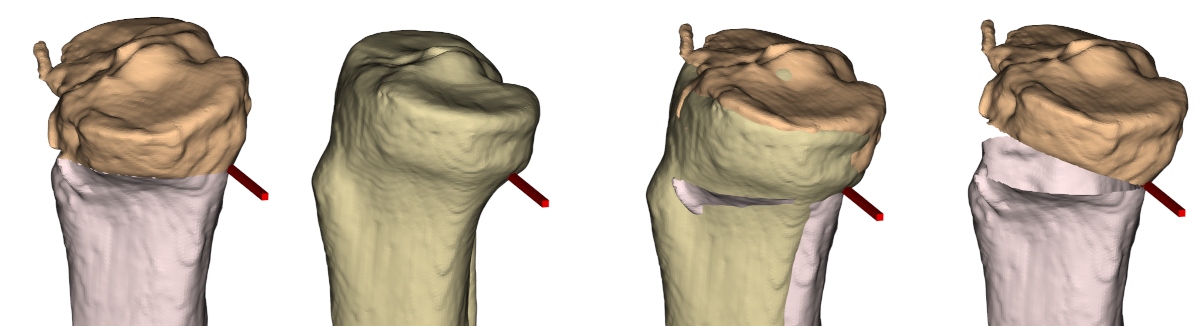
In some cases of hip dislocation, the angle of the femoral head relative to the shaft of the femur is important. Surgery can be performed to rotate the head to a more appropriate angle, but surgeons need to be able to measure the rotation to know how much to move it. We have done some work to show graphically how different methods of measuring the femoral head angle compare.
What shape is the knee?

At the knee we can build models of the patella, allowing us to create more natural patella 'buttons' which replace the worn surface of the kneecap when performing patella-femoral replacement surgery, or total knee replacement surgery. We can also build models of the trochlea that the patella rides in as the knee flexes.
These models can be used to help develop better trochlear implants, providing a more natural track for the patella in the replaced joint.
Hip resurfacing and replacement planning
While total hip replacement is a very successful treatment for osteoarthritis of the hip, and we have options within our planning software for showing the position of a component within the bone, it does often require the removal of an amount of healthy bone, as well as that damaged by disease.
Hip resurfacing can provide a solution that only removes the diseased surface of the bone, retaining the healthy femoral neck and shaft. While metal resurfacing has been available for some time, this has fallen out of favour for many due to problems with metal wear in some manufacturers' components.
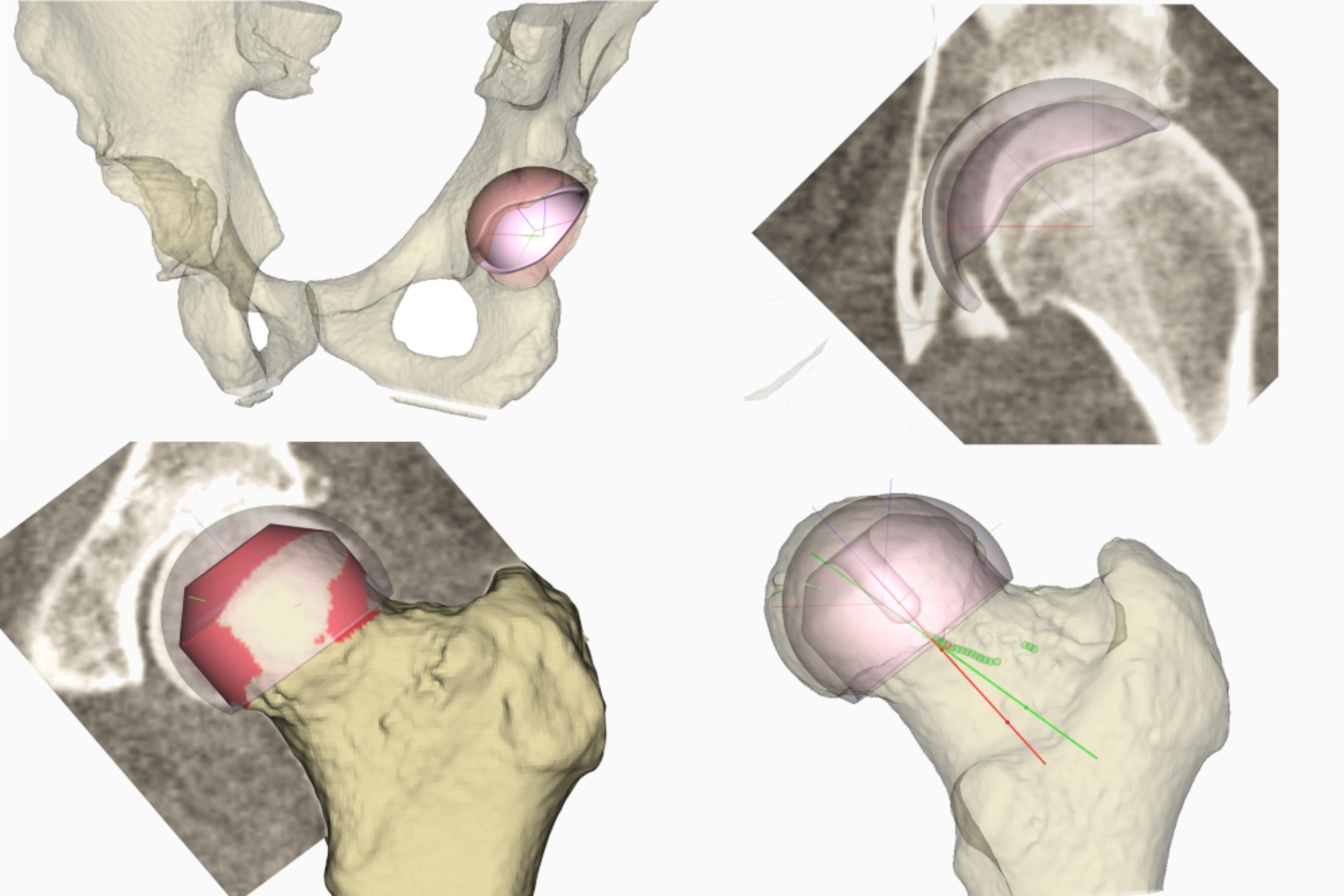
Our spin-out company, Embody, has created a ceramic hip resurfacing system that solves the problem of metal debris, and to aid in the selection and placement of components, we have created a planning system that overlays the ceramic components onto bone, allowing virtual surgery to be performed.
How do we know we got it right?
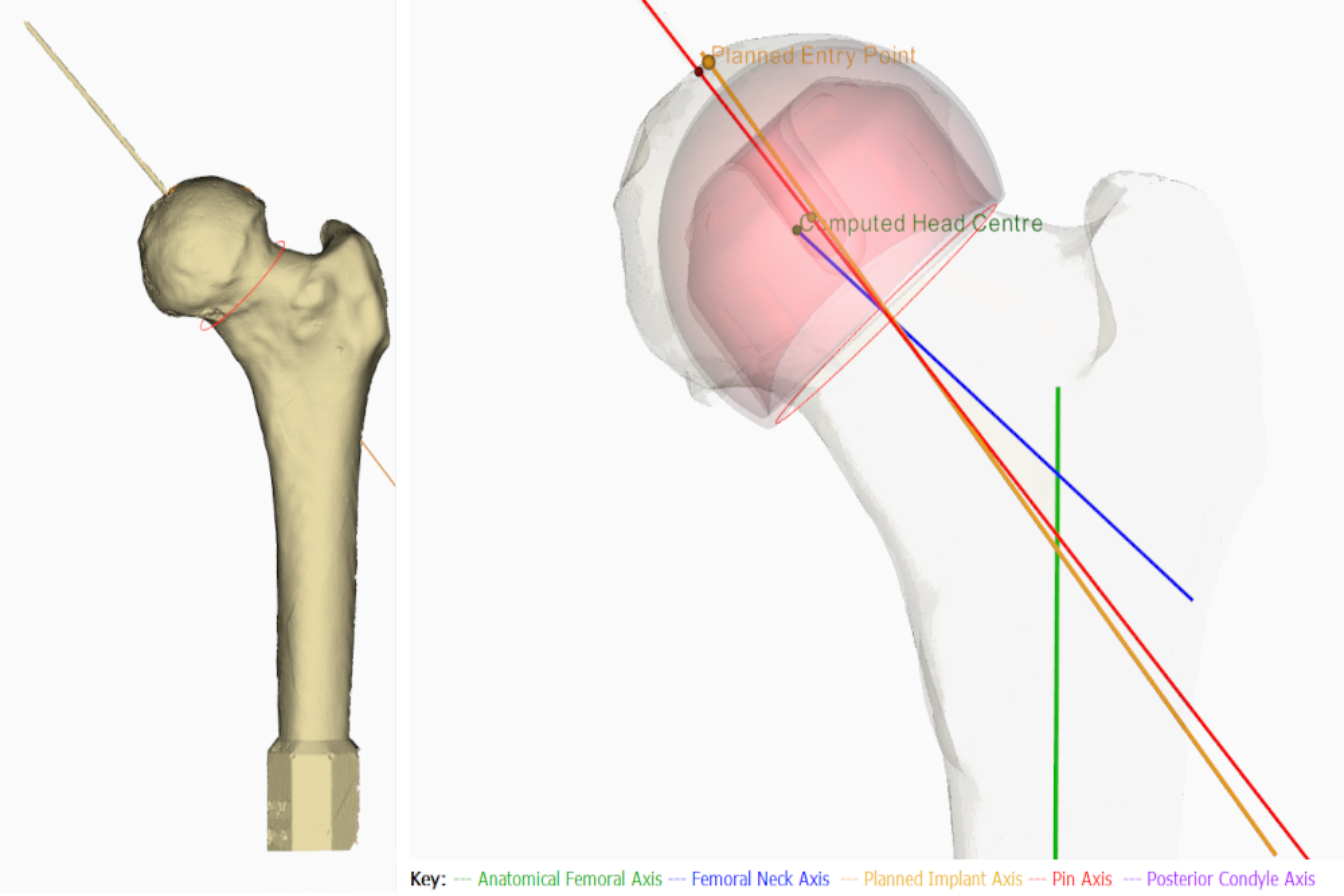
In one study we created foam models of bones from CT scans. We then gave these models to surgeons to insert a guide wire, as they would during surgery using the tools supplied with the implant, into the femoral head. This guide wire sets the orientation of the femoral resurfacing component when placed on the femur. We then laser scanned the bone with the guide wire in place and compared the angle of it to the angle set in the plan.
How much bone did we remove?
We want to preserve as much of the original bone as possible. Often with a joint replacement it is only the surface of the bone that is damaged. We might want to preserve as much of the underlying structure as possible, for example, as insurance in case a revision of the joint replacement is required later in life.
Total and unicompartmental knee replacement planning
Replacing all or part of a worn knee is a very common surgery. While total knee surgery has been performed for many years and can still be the surgery of choice for many, options for less radical surgery are also available where only parts of the knee are replaced.
The knee can be divided into three compartments:
Two where the femur and tibia articulate, and one where the femur and patella (or kneecap) articulate.
Often only one of these is damaged, and in such cases unicompartmental surgery can be performed. Sometimes we can replace two compartments.
Replacing all three compartments is complex surgery, and it's hard to get the balance between each part correct. However, we are creating a planner where individuals or combinations can be replaced using virtual surgery. While technically challenging, there are advantages to this, as the cruciate ligaments are preserved, resulting in a more natural joint motion than for a total knee replacement, and even when all three compartments are replaced, the amount of bone removed is reduced by approximately 50% compared to a total knee replacement.
Osteotomy Planning
In some cases, rather than replacing a joint, the original joint can be retained but realigned. We have looked at osteotomies of the tibia, femur and pelvis to realign knee and hip joints. By planning tibial and femoral osteotomies on the computer, we can determine the best place to make the cuts and the correct angle to realign the bones to create an improved geometry.
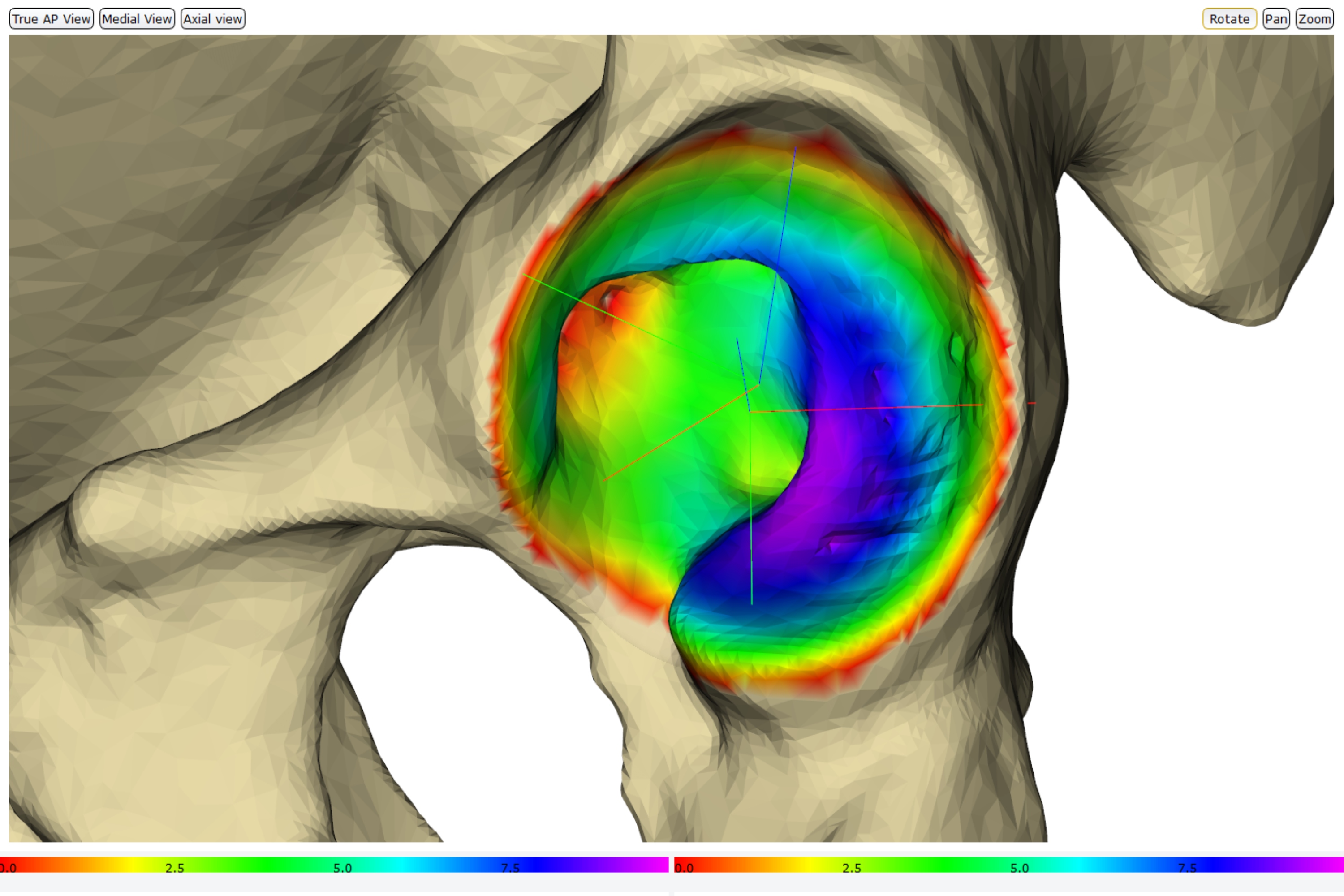
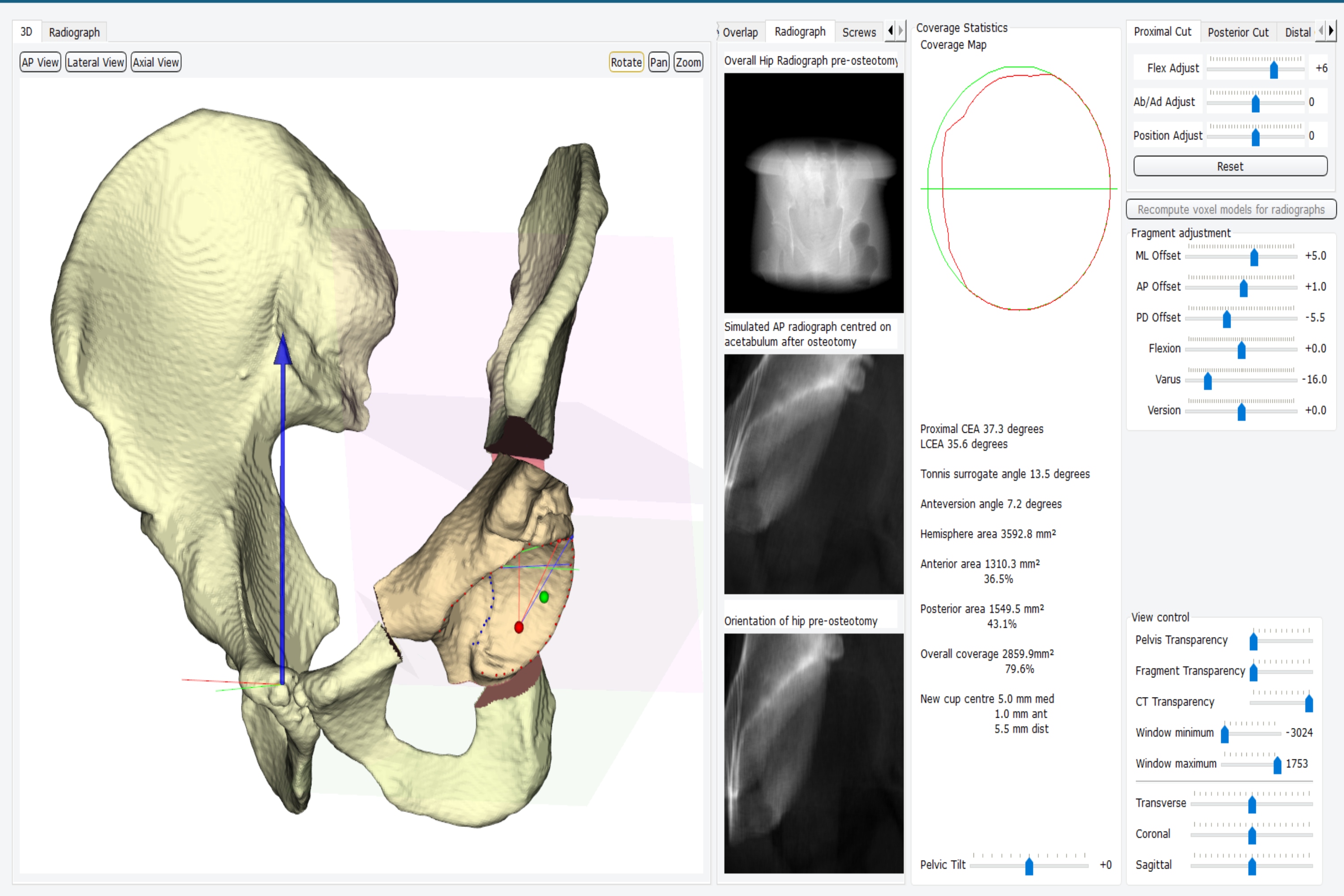
By planning a realignment in the pelvis using what is called a peri-acetabular osteotomy, where the acetabular cup is cut out, realigned and fixed back into place, we can obtain a more stable hip that is less prone to dislocation in patients with hip dysplasia. Real-time feedback while planning provides the surgeon with measurements of the expected improvements in how the relocated cup is covering the head of the femur.
Contact
Dr. Simon Harris
Research Associate
s.harris@imperial.ac.uk