Some breast cancers remain completely resistant to treatment. Now a pioneering two-pronged approach from Imperial offers hope.
Words: Victoria James / Illustration: Matt Murphy
Professor Charles Coombes has been running breast cancer clinics for 40 years. But he is still always moved by the effect of the disease on his patients. “You witness their anxiety as they come to see you, how they’re hoping for their test results to be negative. Everything we’re doing is about reducing that anxiety; we want to save many more lives.”
One in seven women will develop breast cancer in their lifetime, and at a least a quarter of those will face a further frightening challenge – their cancer will become resistant to drug treatment.
Everything we’re doing is about reducing that anxiety; we want to save many more lives."
Professor Charles Coombes
But now a group of Imperial scientists headed by Coombes, Professor of Medical Oncology, and their collaborators at the University of Leicester, are pioneering novel approaches that promise new hope for patients with drug-resistant breast cancer. They are harnessing gene-sequencing technology to usher in a future of wholly individualised treatment.
Treatment for breast cancer used to be – and still can be – gruelling. “In the old days, we used to give chemo, and women would experience sickness, hair loss and bone-marrow failure,” says Coombes. Today, a vast array of targeted drug therapies is available to tackle variant forms of the disease, made possible by both the scale and the ever-evolving tools of cancer research.
Nonetheless, for that unlucky quarter of breast cancer patients, their disease will develop resistance to the prescribed therapy. “There are multiple mechanisms of resistance,” says Coombes. “One common cause is mutation of receptors. These receptors bind oestrogen, inducing gene expression in breast cancer cells that cause them to proliferate.”
Most current treatments work by lowering or blocking oestrogen, so one mechanism of resistance to treatment is when a mutation arises that causes the receptor to be active even in the absence of oestrogen.
The best outcome from treatment is that the cancerous lump is successfully removed, and endocrine therapy kills any cancer cells left in the body. “But there is still a proportion of cases where disease evades treatment,” says Coombes.
“Over time, more aberrations occur in cancer cells and it becomes more difficult to control them. That’s why metastatic disease, where you see the cancer widespread elsewhere in the body, is incurable. The cancer has developed so many aberrations you just can’t control them all.”
With funding help from Cancer Research UK and Innovate UK, the approach of Coombes and his collaborators has been twofold. First, detecting micrometastatic disease ‘on the move’ – that is, catching spreading cancer early. “We had to develop a test that could tell us whether cells are beginning to divide and activate. It’s taken many years, but we’ve done that now. If you take a blood test at regular intervals following surgery and after accessing treatment, you can detect cell-free DNA – that’s fragments of DNA just floating around the blood, which has been excreted when cells die.”
Coombes and his team “interrogate the blood”, looking for mutated cancer DNA variants. Working with colleagues in the US, his team and the Leicester group devised a test that uses detectors individualised for each patient. “You monitor at three months and six months, and in the case of relapse you can see a change in the amount of variant in the blood. We can now detect women becoming resistant to endocrine therapy early and predict when they’re going to relapse. We obviously then want to introduce alternative treatments to prevent that from happening.”
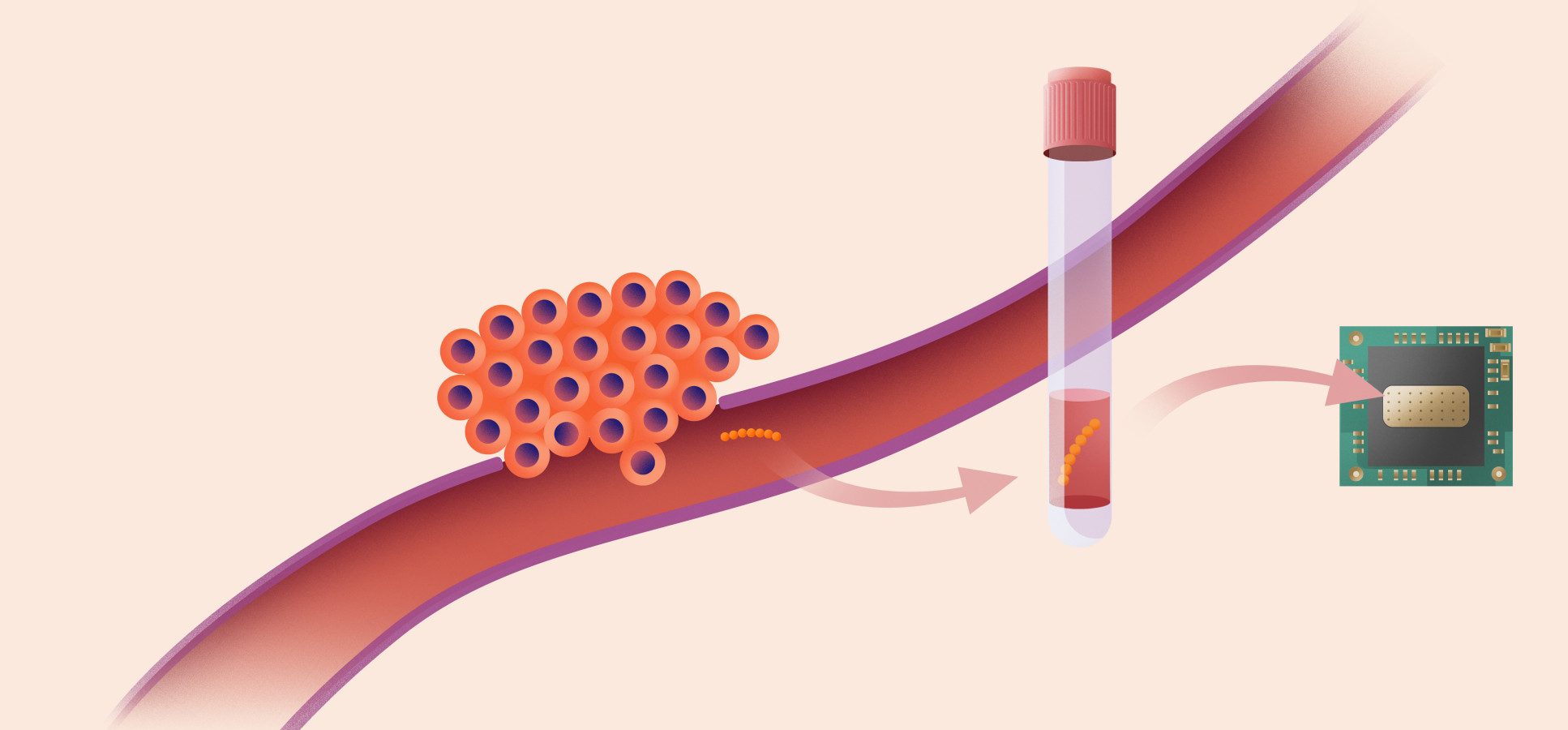
The detection of cell-free DNA
Tumour cells shed cell-free DNA into the blood; Professor Coombes’ team is using patients’ known cancer mutations to develop bespoke assays where these specific mutations can be detected on a microchip. Patients can be tested at three and six months after treatment to check whether the cancer has recurred or is developing resistance to treatment.
Those tests, of course, can be the source of more anxiety for patients, like those Coombes still sees regularly. Which is where Professor Christofer Toumazou, who is Regius Professor of Engineering at Imperial, and his postdoc Melina Kalofonou (MSc Bioengineering 2009, PhD 2013) come in.
“Charles is the most forward-looking oncologist I’ve had the pleasure to meet,” says Toumazou, who is also founder of innovative medical device spinout companies DNA Electronics, or DNAe, and DnaNudge Ltd. “The field we’re involved with is miniaturisation,” he says. “We’re trying to get everything out of the lab and onto a chip.”
Kalofonou, a research fellow and the Cancer Technology Lead for Imperial’s Centre for Bio-inspired Technology, works with patients whose mutations are known, planting reagents for those mutations on a chip, so that when the patients are screened you can identify if that mutation is there.
“The principle is exactly equivalent to what we’re doing with PCR testing for COVID-19,” says Toumazou, “where you know what the genes of the virus are and so can screen people to see if they’ve got it.”
Just as with the Delta and Lambda variants, breast-cancer screening may require detection of multiple known mutations, which requires multiple reagents. But it can all be done on that one chip. “The only ‘lab’ bit is taking a blood sample. You can do it in a GP surgery, with results within an hour while the patient is waiting.”
Chip-based sequencing
Professors Coombes and Toumazou are collaborating to develop a new chip-based sequencing test designed to detect potential mutations that may be present. This approach enables new mutations to also be detected as the disease progresses and, if necessary, different treatment decisions can be made. Chip-based sequencing uses the patient’s cell-free DNA to first create a template which is then bound to a microscopic well on the surface of the microchip.
A complementary strand of DNA is generated against the template by adding different nucleotides, one by one. The incorporation of each nucleotide in the complementary DNA generates an electrical signal that is detected by the chip, indicating which nucleotide is next in the sequence, and thus the full DNA sequence of the template is revealed.
Early detection means early intervention – which is vital when dealing with a disease whose progression can feel like a race against the clock. But Toumazou’s second collaboration with Coombes promises to revolutionise that timeframe. That’s because it gets ahead of the detection of known mutations either by significant multiplexing (DnaNudge) or to the discovery of as-yet unknown mutations (DNAe). “This technology is the sequencing of mutations. Cells mutate differently in different people,” he says. “So, if you just use a testing panel, you will miss something new. But with sequencing you won’t miss it; you’re discovering those mutations in real time.”
The pandemic has accelerated the timeframe within which the group’s work should reach patients. “COVID-19 has opened the door for decentralisation of these technologies,” says Toumazou. “Before, to even think we could run something like this in a GP surgery or through nurses – or even a venue such as health spa, for example – would have seemed fanciful. This discovery and detection was seen as the work of pathologists in laboratories, of centralised labs. But the pandemic has driven decentralisation.”
Toumazou is optimistic about swift adoption. “Before COVID, I would have said it’d take eight to ten years to get this technology out there. But now? A couple of years, maybe less. Charles has the data – he has the key! The constraint now isn’t the platform or the technology, because the technology is here. The constraint is the timeframe for clinical trials.”
Those trials are now getting under way. The pharma companies that have drugs to target many of the cancer proliferation pathways – including AstraZeneca – are working with Coombes and his colleagues, including Professor Jacqui Shaw at the University of Leicester. But Coombes warns that the path ahead isn’t straightforward. “If a woman’s blood test reveals a resistance and you have a drug to target that, you’d think surely you’re going to save that woman. But, sadly, that isn’t always the case. These trials will be very complex, because there are so many different mechanisms that cancer uses to overcome drug treatments – at least a hundred that we know of.”
Despite the challenges ahead, Coombes and Toumazou are confident that the moment has come for their work to break through. “The timing for Charles’s work is being driven by the new wave of decentralisation due to COVID,” says Toumazou. Indeed, Coombes notes that the recent innovations in genomic sequencing couldn’t have changed the game for cancer treatment had they arrived any earlier, because of the scarcity of effective endocrine therapies. “But in the past ten years there has been an explosion of new drugs to target all the different resistance pathways. There are still a few with no decent drug attached, but mostly we’re there.
“One without the other would have been pointless. But right now, it’s a fortunate coming-together of these two strands of research.” Those one in seven women – and the millions more people who love them – will be profoundly grateful for that good timing.